Prevalence of Diabetes Among Obese Adults in Madina, La-Nkwantanang Municipal Assembly and its Immediate Environs
-
Harrison Dzadey
School of Medicine, University of Cape Coast, Cape Coast, Ghana
Patricia Akua YeboahEuropean Institute of Health and Policy, Manchester, United Kingdom
Pamela EzeonyeasiGeoffery Memorial Clinic, Owerri, Nigeria
Genevive Afia Amoakoa AgyapongDepartment of Medical Statistics and Health Data Science, School of Medicine, University of Bristol, Bristol, United Kingdom
Emmanuel Mawuli NattahDepartment of Molecule, Claron Health International, Accra, Ghana
Emmanuel Udochukwu Osisiogu

Department of Science Laboratory Technology, Dr. Hilla Limann Technical University, Wa, Ghana
| Received 14 Apr, 2024 |
Accepted 20 May, 2024 |
Published 21 May, 2024 |
Background and Objective: Obesity and diabetes are escalating public health issues in Africa. Ghana has a high and increasing prevalence of obesity and diabetes, associated with dietary changes, sedentary lifestyles and urbanization. However, most prior studies have focused on urban areas, with limited data on nationwide prevalence, particularly in semi-urban and rural settings. This study aimed to determine the prevalence of diabetes among obese adults in the semi-urban Madina municipality and environs in Ghana. It also examined associated demographic and lifestyle factors. Materials and Methods: This cross-sectional study surveyed 106 obese adults aged ≥18 years in Madina using questionnaires and anthropometric measurements. Fasting blood sugar (FBS) was measured to assess diabetes status. Data was analyzed using the Statistical Package for Social Sciences (SPSS). Results were computed in graphs and tables using Microsoft Office. Results: Most participants were urban, female, single and educated to at least a basic level. Diabetes prevalence was 15% based on elevated FBS. The highest prevalence was among those with basic education (19%) and the lowest was in students (5%). Diabetes was more common in urban residents (15%) than in rural (17%) or peri-urban (16%). High diabetes prevalence was found in those engaged in trading (26%) and self-employment (22%). Diets high in refined carbohydrates are associated with poorer blood sugar control. A family history of diabetes and hypertension was a risk factor for high FBS. Conclusion: Diabetes prevalence was signific ant among obese adults in this semi-urban region of Ghana. Lower education, urban residence, unhealthy diets, family history and occupations like trading confer higher diabetes risk. Preventive interventions should target these vulnerable subgroups.
| Copyright © 2024 Dzadey et al. This is an open-access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. |
INTRODUCTION
The global prevalence of obesity and diabetes has risen significantly in recent decades. According to 2016 estimates by the World Health Organization (WHO), over 1.9 billion adults worldwide are overweight and 650 million are obese1. Obesity is a major risk factor for type 2 diabetes, accounting for 80-85% of the overall risk2. The number of adults with diabetes has quadrupled since 1980 to 422 million, with prevalence doubling in middle- and low-income countries1. In Africa, diabetes prevalence has increased concurrently with rising obesity rates over the past decade, presenting major public health challenges3,4 Dietary changes, sedentary lifestyles and urbanization have been cited as key drivers of escalating obesity and diabetes trends on the continent5.
In Ghana, the prevalence of obesity in adults was estimated to be 14.1% in 2003, with higher rates among females6. Diabetes affects approximately 6% of Ghanaian adults, with age and obesity as predisposing risk factors7. Another study found overweight and obesity prevalence of 23% among Ghanaian adults, associated with advanced age, female gender, urban residence, high income and education levels8. However, there remains limited research on the correlation between obesity indices like Body Mass Index (BMI), waist circumference and waist-hip ratio with diabetes risks in Ghana. Further studies have recommended investigating these anthropometric measures to elucidate the pathogenesis of diabetes to obesity9.
Socioeconomic factors like education, occupation, diet and physical activity also need to be assessed to identify high-risk populations for targeted preventive interventions10. Most prior studies on obesity and diabetes in Ghana have been limited to urban settings7,11. There is a lack of research on nationwide prevalence, particularly in semi-urban and rural areas. Therefore, this study aimed to determine the prevalence of diabetes among obese adults in the Madina municipality and environs in Ghana. It also examined associated demographic factors like gender, age, residence, education, occupation, diet, physical activity and family history.
MATERIALS AND METHODS
Study site: The study was carried out in Madina and its environs from January to June, 2022. The La-Nkwantanang-Madina Municipal is one of the 261 Metropolitan, Municipal and District Assemblies (MMDAs) in Ghana and forms part of the 29 MMDAs in the Greater Accra Region. The population of the Municipality according to the 2021 population and housing census stands at 244,676 with 120,846 males and 123,830 females12.
Study design: The study followed a cross-sectional pattern within Madina and its environs and questionnaires were administered to obtain information that was used in this study.
Sample size and sample population: The sample size for this study was 106 participants. The population was obese adults aged 18 years and above in Madina and its immediate environs.
Sampling technique: A standard questionnaire was used to collect information on the socio-demography and participants’ profiles such as age, sex and family history of diabetes. Random sampling was used for the study.
Physical measurements: Body weight and height were checked using a standard scale and stadiometer to calculate the Body Mass Index (BMI). The waist-hip ratio was measured at the approximate midpoint between the lower margin of the last palpable rib and the top of the iliac crest13. Thus, three anthropometric proxies of obesity were used; (BMI) ≥30 kg/m2, waist circumference (WC) ≥88 cm and waist-hip ratio (WHR) ≥0.85 cm14.
Biochemical analysis
Fasting blood sugar test: Blood sample was taken after an overnight fast to determine the body’s glucose level. A fasting plasma glucose greater than or equal to 7.0 mmol/L (126 mg/dL) was indicative of diabetes as described by WHO and the American Diabetes Association (ADA) criteria for diabetes diagnosis15,16.
Statistical analysis: Data obtained was analyzed using the Statistical Package for Social Sciences (SPSS) version 20. Results were computed in graphs and tables using Microsoft Office package 2010.
RESULTS AND DISCUSSION
The diabetic participants were predominantly urban, female, single and educated to at least a basic level. Trading was the most frequent occupation reported. Table 1 provides useful demographic context on the study population.
The majority of the 106 participants had either a tertiary (39), basic (42) or secondary (20) education, with very few (5) having no education. Across all education levels, females greatly outnumbered males, especially in the tertiary education group where there were 34 females versus just 5 males. Regarding diabetes status, most participants in each education bracket had a normal FBS rather than a high FBS indicative of low diabetes prevalence. However, the basic education group had the highest number (8) of participants with a high FBS indicative of uncontrolled diabetes. Very few participants currently smoked or previously smoked, across education levels and genders. More participants currently consumed alcohol or previously consumed alcohol compared to smoking.
Although normal FBS levels were more prevalent among current alcohol drinkers, a high FBS was also more common among current alcohol drinkers, especially those with basic education. The basic education group again had the most cases (3) of a high FBS indicative of diabetes who were current alcohol drinkers. For water intake, most participants frequently drank water rather than being infrequent water drinkers, however, the tertiary education group had the most infrequent drinkers (3). Table 2 provides more details of the analysis.
| Table 1: | A table showing the distribution of demographic characteristics of the diabetic population | |||
| Variable | Category | Frequency | Percent |
| Gender | Female | 91 | 85.8 |
| Male | 15 | 14.2 | |
| Residence | Urban | 68 | 64.2 |
| Rural | 6 | 5.7 | |
| Peri-urban | 32 | 30.2 | |
| Marital | Married | 42 | 39.6 |
| status | Divorced | 6 | 5.7 |
| Single | 56 | 52.8 | |
| Widowed | 2 | 1.9 | |
| Educational | Tertiary | 39 | 36.8 |
| status | Secondary | 20 | 18.9 |
| Basic | 42 | 39.6 | |
| No education | 5 | 4.7 | |
| Occupation | Formal sector | 12 | 11.3 |
| Self employed | 23 | 21.7 | |
| Student | 22 | 20.8 | |
| Trading | 43 | 40.6 | |
| Unemployed | 6 | 5.7 |
| Table 2: | Comparison between education, gender, diabetes status and other variables | |||
| FBS interpretation |
Currently smoke? |
Smoked before? |
Currently drink? |
Drank alcohol before? |
Frequently drink water |
|||||||
| Education | Gender | High | Normal | No | Yes | No | Yes | No | Yes | No | Yes | No |
| Tertiary | Female | 4 | 24 | 28 | 2 | 26 | 6 | 22 | 14 | 14 | 26 | 2 |
| Male | 1 | 10 | 11 | 2 | 9 | 5 | 6 | 7 | 4 | 10 | 1 | |
| Total | 5 | 34 | 39 | 4 | 35 | 11 | 28 | 21 | 18 | 36 | 3 | |
| Secondary | Female | 1 | 18 | 19 | 1 | 18 | 5 | 14 | 11 | 8 | 17 | 2 |
| Male | 0 | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | |
| Total | 1 | 19 | 20 | 1 | 19 | 6 | 14 | 12 | 8 | 18 | 2 | |
| Basic | Female | 7 | 32 | 39 | 0 | 39 | 19 | 20 | 30 | 9 | 38 | 1 |
| Male | 1 | 2 | 3 | 0 | 3 | 1 | 2 | 3 | 0 | 3 | 0 | |
| Total | 8 | 34 | 42 | 0 | 0 | 20 | 22 | 33 | 9 | 41 | 1 | |
| No education | Female | 2 | 3 | 5 | 0 | 5 | 1 | 4 | 4 | 1 | 4 | 1 |
| Total | 2 | 3 | 5 | 0 | 0 | 1 | 4 | 4 | 1 | 4 | 1 | |
| Total | Female | 14 | 77 | 91 | 3 | 88 | 31 | 60 | 59 | 32 | 85 | 6 |
| Male | 2 | 13 | 15 | 2 | 13 | 7 | 8 | 11 | 4 | 14 | 1 | |
| Total | 16 | 90 | 106 | 5 | 101 | 38 | 68 | 70 | 36 | 99 | 7 | |
| Table 3: | Comparison between education, gender, exercise and family history | |||
| Exercise | Family history | |||||||
| Education | Gender | Regularly | Sometimes | Never | Diabetes | Diabetes and Hypertension |
hypertension | None |
| Tertiary | Female | 3 | 17 | 8 | 5 | 5 | 5 | 13 |
| Male | 1 | 6 | 4 | 1 | 1 | 4 | 5 | |
| Total | 4 | 23 | 12 | 6 | 6 | 9 | 18 | |
| Secondary | Female | 1 | 9 | 9 | 4 | 6 | 1 | 8 |
| Male | 0 | 1 | 0 | 1 | 0 | 0 | 0 | |
| Total | 1 | 10 | 9 | 5 | 6 | 1 | 8 | |
| Basic | Female | 3 | 15 | 21 | 5 | 7 | 8 | 19 |
| Male | 0 | 2 | 1 | 1 | 1 | 0 | 1 | |
| Total | 3 | 17 | 22 | 6 | 8 | 8 | 20 | |
| No education | Female | 0 | 1 | 0 | 0 | 0 | 0 | 3 |
| Total | 0 | 1 | 4 | 0 | 2 | 0 | 3 | |
Most participants exercised either “sometimes” or “never” rather than regularly, across all education brackets and genders. Those with tertiary education had the highest number (4) who exercised regularly. Around half of participants overall had no family history of diabetes or hypertension. The tertiary education group had the highest number (18) with no family history. The basic education group had the most cases (8) of family history of both diabetes and hypertension. More females exercised sometimes or never compared to males across education levels. Slightly more males had a family history of diabetes or hypertension than females.
Regular exercise decreased with lower education level, with 4 in tertiary education exercising regularly, 1 in secondary and 3 in basic education. Family history of diabetes and hypertension was highest in the basic education group (8), followed by tertiary education (6). Irregular exercise and a family history of chronic health conditions were conspicuously common in this study (Table 3). Those with lower education levels exercised less regularly but had a higher family history of diabetes and hypertension. This indicates physical inactivity and genetic predisposition may contribute to diabetes risks among those with lower education. The trends further reinforce associations noted between lower education and poorer diabetes control.
| Table 4: | Comparison between education, residence, diabetes status and other variables | |||
| FBS interpretation |
Currently smoke? |
Smoked before? |
Currently drink? |
Drank alcohol before? |
Frequently drink water? |
|||||||
| Education | Residence | High | Normal | No | Yes | No | Yes | No | Yes | No | Yes | No |
| Tertiary | Urban | 5 | 25 | 30 | 3 | 27 | 10 | 20 | 17 | 13 | 27 | 3 |
| Rural | 0 | 2 | 2 | 0 | 2 | 0 | 2 | 2 | 0 | 2 | 0 | |
| Peri-urban | 0 | 7 | 7 | 1 | 6 | 1 | 6 | 2 | 5 | 7 | 0 | |
| Total | 5 | 34 | 39 | 4 | 35 | 11 | 28 | 21 | 18 | 36 | 3 | |
| Secondary | Urban | 0 | 15 | 15 | 0 | 15 | 5 | 10 | 9 | 6 | 14 | 1 |
| Peri-urban | 1 | 4 | 5 | 1 | 4 | 1 | 4 | 3 | 2 | 4 | 1 | |
| Total | 1 | 19 | 20 | 1 | 19 | 6 | 14 | 12 | 8 | 18 | 2 | |
| Basic | Urban | 5 | 17 | 22 | 22 | 12 | 10 | 17 | 5 | 22 | 0 | |
| Rural | 1 | 2 | 3 | 3 | 1 | 2 | 3 | 0 | 3 | 0 | ||
| Peri-urban | 2 | 15 | 17 | 17 | 7 | 10 | 13 | 4 | 16 | 1 | ||
| Total | 8 | 34 | 42 | 42 | 20 | 22 | 33 | 9 | 41 | 1 | ||
| No education | Urban | 0 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | |
| Rural | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | ||
| Peri-urban | 2 | 1 | 3 | 3 | 0 | 3 | 2 | 1 | 3 | 0 | ||
| Total | 2 | 3 | 5 | 5 | 1 | 4 | 4 | 1 | 4 | 1 | ||
| Total | Urban | 10 | 58 | 68 | 3 | 65 | 27 | 41 | 44 | 24 | 63 | 5 |
| Rural | 1 | 5 | 6 | 0 | 6 | 2 | 4 | 6 | 0 | 6 | 0 | |
| Peri-urban | 5 | 27 | 32 | 2 | 30 | 9 | 23 | 20 | 12 | 30 | 2 | |
| Total | 16 | 90 | 106 | 5 | 101 | 38 | 68 | 70 | 36 | 99 | 7 | |
Most participants resided in urban areas across all education levels, especially those with tertiary education where 30 out of 39 lived in cities17. Those with basic education in urban areas had the highest number (5) with uncontrolled high blood sugar (2). Very few participants currently or previously smoked, irrespective of education, residence or gender18. More participants currently or previously consumed alcohol than smoked tobacco19. High blood sugars were more prevalent among urban residents who currently drink alcohol20.
The basic education group again had the most urban cases (3) of high blood sugar who currently drink21. Most participants frequently drank water, although tertiary educated urban residents had the highest number (3) of infrequent drinkers (9). Basic educated urban dwellers exhibited the highest rates of uncontrolled high blood sugar indicative of diabetes. High blood sugar was also more prevalent among urban alcohol drinkers, especially those with basic education (Table 4).
Most of the participants exercised irregularly or never across all educational levels and residence groups22. However, tertiary educated urban dwellers had the highest number (4) who exercised regularly (2). Basic educated rural residents had the highest number (1) with a family history of both diabetes and hypertension23. More urban females exercised irregularly compared to rural females across educational levels7,24. Regular exercise was lowest in rural areas24,25.
Family history of both conditions was highest amongst urban tertiary educated (8) followed by basic education urban residents25-27. Infrequent exercise and a family history of chronic health conditions were common, especially in urban areas in this study. Rural residents with basic education had poorer exercise habits but a higher dual family history (Table 5). This indicates inactivity and genetics may increase diabetes risks, particularly for basic educated rural populations9,27,28.
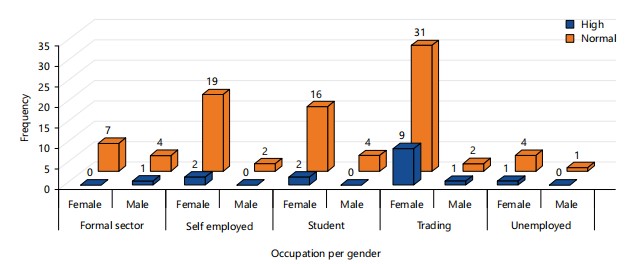
The majority of participants in each occupation had normal blood sugar rather than high blood sugar indicative of low diabetes prevalence, regardless of gender. However, elevated levels were most prevalent among females engaged in trading and males who were self-employed. In contrast, students had the lowest rates of high blood sugar. Unemployed participants and those in the formal sector also exhibited better blood sugar control (Fig. 1).
These trends suggest trading roles and self-employment may be linked to poorer diabetes regulation, likely due to associated lifestyle factors. Similar studies in urban Africa have found high diabetes prevalence among traders and entrepreneurs attributed to unhealthy diets and physical inactivity27-29. Given many traders and self-employed individuals in urban Ghana are low-income earners, financial barriers to healthy lifestyles may increase their diabetes risks29,30.
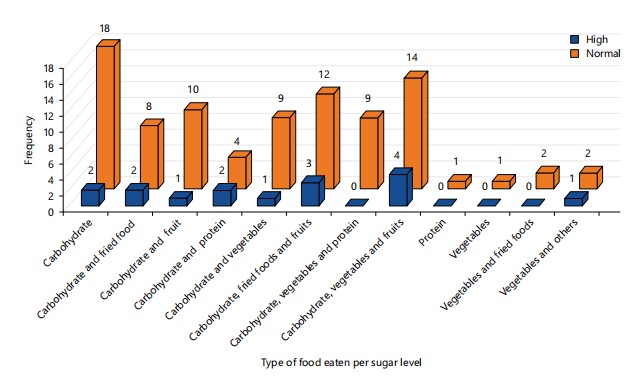
Overall, most individuals had normal blood sugar rather than elevated high levels regardless of diet. However, high blood sugar was most frequent among those consuming carbohydrate-rich foods like kenkey (8 high vs 10 normal) and banku (4 high vs 9 normal). In contrast, participants eating protein-rich foods like fish (0 high vs 4 normal) and eggs (1 high vs 2 normal) exhibited better blood sugar control.
| Table 5: | Comparison between education, residence, family history and exercise | |||
| Family history | Exercise | |||||||
| Education | Residence | Diabetes | Hypertension | Diabetes and hypertension |
None | Regularly | Sometimes | Never |
| Tertiary | Urban | 4 | 3 | 8 | 15 | 4 | 15 | 11 |
| Rural | 1 | 1 | 0 | 0 | 0 | 2 | 0 | |
| Peri-urban | 1 | 2 | 1 | 3 | 0 | 6 | 1 | |
| Total | 6 | 6 | 9 | 18 | 4 | 23 | 12 | |
| Secondary | Urban | 5 | 6 | 0 | 4 | 0 | 7 | 8 |
| Peri-urban | 0 | 0 | 1 | 4 | 1 | 3 | 1 | |
| Total | 5 | 6 | 1 | 8 | 1 | 10 | 9 | |
| Basic | Urban | 2 | 6 | 4 | 10 | 1 | 9 | 12 |
| Rural | 1 | 1 | 0 | 1 | 0 | 0 | 3 | |
| Peri-urban | 3 | 1 | 4 | 9 | 2 | 8 | 7 | |
| Total | 6 | 8 | 8 | 20 | 3 | 17 | 22 | |
| No education | Urban | 0 | 1 | 0 | 0 | 0 | 0 | 1 |
| Rural | 0 | 1 | 0 | 0 | 0 | 0 | 1 | |
| Peri-urban | 0 | 0 | 0 | 3 | 0 | 1 | 2 | |
| Total | 0 | 2 | 0 | 0 | 0 | 0 | 4 | |
| Total | Urban | 11 | 16 | 12 | 29 | 5 | 31 | 32 |
| Rural | 2 | 3 | 0 | 1 | 0 | 2 | 4 | |
| Peri-urban | 4 | 3 | 6 | 19 | 3 | 18 | 11 | |
| Total | 17 | 22 | 18 | 49 | 8 | 51 | 47 | |
|
|
|
These findings concur with other African studies showing high carbohydrate diets, especially refined grains, associated with poorer glycemic regulation in urban diabetics30,31. In comparison, increased intake of foods like fish and eggs may improve diabetes outcomes31-33. The high carbohydrate diets predominant in urban Ghana likely contribute to rising diabetes prevalence by promoting postprandial hyperglycemia33,34. As such, reducing refined carbohydrate consumption and increasing protein intake should be a focus of lifestyle interventions for the growing number of urban diabetics in Ghana. Figure 2 compares dietary habits with fasting blood sugar levels among the diabetic study participants.
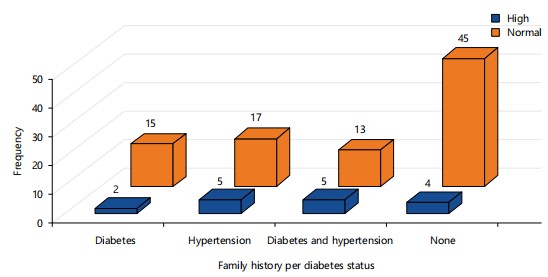
Overall, most individuals had normal blood sugar levels regardless of family history. However, high blood sugar indicative of diabetes was most frequent among those with a family history of both diabetes and hypertension. These findings concurred with other studies in Ghanaians showing genetic predisposition to chronic diseases like diabetes is common and associated with poorer glycemic regulation7,35.
The high rates of family history of metabolic disorders likely contribute to escalating diabetes prevalence in Ghana through increased genetic susceptibility, particularly when coupled with obesogenic lifestyles35. As such, diabetes prevention efforts should target individuals with a family history of chronic diseases like hypertension, given their higher risk for developing uncontrolled hyperglycemia. Lifestyle and pharmacological interventions may help prevent or delay diabetes onset in this genetically predisposed population. Figure 3 compares family history of diabetes, hypertension or both conditions with current diabetes status among the participants. The findings can help guide policies and programs to curb escalating obesity and diabetes in Ghana through risk factor modification and lifestyle interventions.
CONCLUSION
This study found a 15% prevalence of diabetes among obese adults in the semi-urban Madina municipality and environs of Ghana. The highest diabetes prevalence was observed among those with basic education and urban dwellers, especially traders and the self-employed. Diets high in refined carbohydrates were associated with poorer blood sugar control compared to protein-rich foods. Genetic predisposition to chronic diseases also contributed to uncontrolled hyperglycemia.
SIGNIFICANCE STATEMENT
This study aimed to determine the prevalence of diabetes among obese adults in the Madina municipality and environs of Ghana, examining associated demographic and lifestyle factors. The results showed a 15% prevalence of diabetes in this population. Diabetes was more prevalent among those with lower education levels, urban residents, unhealthy dietary habits high in refined carbohydrates, occupations like trading and those with a family history of chronic diseases like diabetes and hypertension. The findings highlight vulnerable subgroups requiring targeted interventions to promote healthy lifestyles and prevent the escalating burden of obesity and diabetes in Ghana.
The significant burden of diabetes in this semi-urban region highlights the need for preventive strategies nationwide, not just in urban cities. Lower-educated, urban-dwelling traders with a family history of metabolic disorders are at high risk and should be targeted for lifestyle interventions promoting healthy diets, regular exercise and weight control. Addressing financial barriers to healthy lifestyles for low-income groups is also essential. At the national level, policies and programs are needed to curb the rising prevalence of obesity and diabetes across Ghana. This includes regulating the food industry, education campaigns, screening initiatives and improving access to diabetes care. Without concerted prevention efforts, the escalating non-communicable disease epidemic threatens progress and imposes substantial social and economic burdens. The findings from this semi-urban area provide insights to guide further research and interventions tailored to the needs of vulnerable subgroups in Ghana.
ACKNOWLEDGMENT
The authors of this study wish to acknowledge all participants who took part in this study. The careful reading and constructive feedback from anonymous reviewers significantly improved the quality of this manuscript and thus we are grateful to them all.
REFERENCES
- Bhupathiraju, S.N. and F.B. Hu, 2016. Epidemiology of obesity and diabetes and their cardiovascular complications. Circ. Res., 118: 1723-1735.
- Bosu, W.K., 2015. An overview of the nutrition transition in West Africa: Implications for non-communicable diseases. Proc. Nutr. Soc., 74: 466-477.
- Shaw, J.E., R.A. Sicree and P.Z. Zimmet, 2010. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res. Clin. Pract., 87: 4-14.
- Essien, O., A. Otu, V. Umoh, O. Enang, J.P. Hicks and J. Walley, 2017. Intensive patient education improves glycaemic control in diabetes compared to conventional education: A randomised controlled trial in a Nigerian tertiary care hospital. PLoS ONE, 12.
- Adeloye, D., J.O. Ige, A.V. Aderemi, N. Adeleye, E.O. Amoo, A. Auta and G. Oni, 2017. Estimating the prevalence, hospitalisation and mortality from type 2 diabetes mellitus in Nigeria: A systematic review and meta-analysis. BMJ Open, 7.
- Amoah, A.G.B., 2003. Obesity in adult residents of Accra, Ghana. Ethnicity Dis., 13: 97-101.
- Danquah, I., G. Bedu-Addo, K.J. Terpe, F. Micah and Y.A. Amoako et al., 2012. Diabetes mellitus type 2 in urban Ghana: Characteristics and associated factors. BMC Public Health, 12.
- Duda, R.B., R. Darko, J. Seffah, R.M. Adanu, J.K. Anarfi and A.G. Hill, 2007. Prevalence of obesity in women of Accra, Ghana. Afr. J. Health Sci., 14: 154-159.
- Baatiema, L., A. de-Graft Aikins, A. Sav, G. Mnatzaganian and C.K.Y. Chan and S. Somerset, 2017. Barriers to evidence-based acute stroke care in Ghana: A qualitative study on the perspectives of stroke care professionals. BMJ Open, 7.
- Ofori-Asenso, R., A.A. Agyeman, A. Laar and D. Boateng, 2016. Overweight and obesity epidemic in Ghana-A systematic review and meta-analysis. BMC Public Health, 16.
- Agyei-Mensah, S. and A. de-Graft Aikins, 2010. Epidemiological transition and the double burden of disease in Accra, Ghana. J. Urban Health, 87: 879-897.
- Agyekum, M.W., G.F. Afrifa-Anane and F. Kyei-Arthur, 2024. Prevalence and correlates of disability in older adults, Ghana: Evidence from the Ghana 2021 population and housing census. BMC Geriatr., 24.
- Nishida, C., G.T. Ko and S. Kumanyika, 2010. Body fat distribution and noncommunicable diseases in populations: Overview of the 2008 WHO Expert Consultation on Waist Circumference and Waist-Hip Ratio. Eur. J. Clin. Nutr., 64: 2-5.
- Moore, J.B., J.C. Hanes, P. Barbeau, B. Gutin, R.P. Treviño and Z. Yin, 2007. Validation of the physical activity questionnaire for older children in children of different races. Pediatr. Exercise Sci., 19: 6-19.
- Amoah, A.G.B., S.K. Owusu and S. Adjei, 2002. Diabetes in Ghana: A community based prevalence study in greater Accra. Diabetes Res. Clin. Pract., 56: 197-205.
- ADAPPC, 2022. Classification and diagnosis of diabetes: Standards of medical care in diabetes-2022. Diabetes Care, 45: S17-S38.
- Haregu, T.N., G. Setswe, J. Elliott and B. Oldenburg, 2014. National responses to HIV/AIDS and non-communicable diseases in developing countries: Analysis of strategic parallels and differences. J. Public Health Res., 3.
- Oyewole, B.K., V.J. Animasahun and H.J. Chapman, 2018. Tobacco use in Nigerian youth: A systematic review. PLoS ONE, 13.
- Peltzer, K., S. Pengpid, T.A. Samuels, N.K. Özcan and C. Mantilla et al., 2014. Prevalence of overweight/obesity and its associated factors among university students from 22 countries. Int. J. Environ. Res. Public Health, 11: 7425-7441.
- Peer, N., K. Steyn, C. Lombard, E.V. Lambert, B. Vythilingum and N.S. Levitt, 2012. Rising diabetes prevalence among urban-dwelling black South Africans. PLoS ONE, 7.
- de-Graft Aikins, A., P. Boynton and L.L. Atanga, 2010. Developing effective chronic disease interventions in Africa: Insights from Ghana and Cameroon. Global Health, 6.
- Ojofeitimi, E.O., A.O. Adeyeye, A.O. Fadiora, A.O. Kuteyi and T.G. Faborode et al., 2007. Awareness of obesity and its health hazard among women in a university community. Pak. J. Nutr., 6: 502-505.
- Arrey, W.T., C.A. Dimala, J. Atashili, J. Mbuagbaw and G.L. Monekosso, 2016. Hypertension, an emerging problem in rural Cameroon: Prevalence, risk factors, and control. Int. J. Hypertens., 2016.
- Kumah, D.B., K.O. Akuffo, J.E. Abaka-Cann, D.E. Affram and E.A. Osae, 2015. Prevalence of overweight and obesity among students in the Kumasi metropolis. J. Nutr. Metab., 2015.
- Price, A.J., A.C. Crampin, A. Amberbir, N. Kayuni-Chihana and C. Musicha et al., 2018. Prevalence of obesity, hypertension, and diabetes, and cascade of care in Sub-Saharan Africa: A cross-sectional, population-based study in rural and urban Malawi. Lancet Diabetes Endocrinol., 6: 208-222.
- Sifunda, S., A.D. Mbewu, M. Mabaso, T. Manyaapelo and R. Sewpaul et al., 2023. Prevalence and psychosocial correlates of diabetes mellitus in South Africa: Results from the South African National Health and Nutrition Examination Survey (SANHANES-1). Int. J. Environ. Res. Public Health, 20.
- Mbanya, J.C.N., A.A. Motala, E. Sobngwi, F.K. Assah and S.T. Enoru, 2010. Diabetes in Sub-Saharan Africa. Lancet, 375: 2254-2266.
- Aspray, T.J., F. Mugusi, S. Rashid, D. Whiting, R. Edwards, K.G. Alberti and N.C. Unwin, 2000. Rural and urban differences in diabetes prevalence in Tanzania: The role of obesity, physical inactivity and urban living. Trans. R. Soc. Trop. Med. Hyg., 94: 637-644.
- Acquah, D., E.A. Oduro, P. Adoba, H. Agbodzakay, J. Kyei-Mensah and R.K. Ephraim, 2018. Hyperglycemia in rural dwellers: A cross sectional study of the Effutu Municipality, Ghana. Integr. Diabetes Cardiovasc. Dis., 3: 67-71.
- Chen, L.L., A.F.M. Ludin, S. Shahar, Z.A. Manaf and N.M. Tohit, 2020. Meal replacement in dietary management of type-2 diabetes mellitus: A scoping review protocol. Syst. Rev., 9.
- Lee, J. and J. Kim, 2018. Egg consumption is associated with a lower risk of type 2 diabetes in middle-aged and older men. Nutr. Res. Pract., 12: 396-405.
- Xun, P. and K. He, 2012. Fish consumption and incidence of diabetes: Meta-analysis of data from 438,000 individuals in 12 independent prospective cohorts with an average 11-year follow-up. Diabetes Care, 35: 930-938.
- Clifton, P.M., L.T. Coles and C.E. Galbraith, 2016. Low carbohydrate diets in type 2 diabetes-A translational study. J. Diabetes Mellitus, 6: 152-157.
- Djrolo, F., T. Adoukonou, C. Houehanou, J.D. Houinato and D. Houinato, 2015. Diabetes in Borgou Department in Benin: Prevalence and associated factors. J. Diabetes Mellitus, 5: 90-96.
- Agyemang, C., K. Meeks, E. Beune, E. Owusu-Dabo and F.P. Mockenhaupt et al., 2016. Obesity and type 2 diabetes in Sub-Saharan Africans-Is the burden in today's Africa similar to African migrants in Europe? The RODAM study. BMC Med., 14.
How to Cite this paper?
APA-7 Style
Dzadey,
H., Yeboah,
P.A., Ezeonyeasi,
P., Agyapong,
G.A., Nattah,
E.M., Osisiogu,
E.U. (2024). Prevalence of Diabetes Among Obese Adults in Madina, La-Nkwantanang Municipal Assembly and its Immediate Environs. Science International, 12(1), 1-10. https://doi.org/10.17311/sciintl.2024.01.10
ACS Style
Dzadey,
H.; Yeboah,
P.A.; Ezeonyeasi,
P.; Agyapong,
G.A.; Nattah,
E.M.; Osisiogu,
E.U. Prevalence of Diabetes Among Obese Adults in Madina, La-Nkwantanang Municipal Assembly and its Immediate Environs. Sci. Int 2024, 12, 1-10. https://doi.org/10.17311/sciintl.2024.01.10
AMA Style
Dzadey
H, Yeboah
PA, Ezeonyeasi
P, Agyapong
GA, Nattah
EM, Osisiogu
EU. Prevalence of Diabetes Among Obese Adults in Madina, La-Nkwantanang Municipal Assembly and its Immediate Environs. Science International. 2024; 12(1): 1-10. https://doi.org/10.17311/sciintl.2024.01.10
Chicago/Turabian Style
Dzadey, Harrison, Patricia Akua Yeboah, Pamela Ezeonyeasi, Genevive Afia Amoakoa Agyapong, Emmanuel Mawuli Nattah, and Emmanuel Udochukwu Osisiogu.
2024. "Prevalence of Diabetes Among Obese Adults in Madina, La-Nkwantanang Municipal Assembly and its Immediate Environs" Science International 12, no. 1: 1-10. https://doi.org/10.17311/sciintl.2024.01.10

This work is licensed under a Creative Commons Attribution 4.0 International License.